
Electronic Apex Locator vs Radiographs for Working Length Determination
Introduction – Why Compare Electronic Apex Locators and Radiographs?
Determining precise working length (WL) is foundational to endodontic success. While clinicians historically relied on conventional radiographs, modern practice has shifted toward electronic apex locators (EALs). Recent 2024–2025 systematic reviews have reignited this debate: Alarifi (2025) reports that EALs achieve acceptable WL in up to 92% of cases—significantly outperforming radiography—while Kaur (2024) emphasizes that evidence certainty remains a subject of ongoing scrutiny.
This comparison addresses a vital question: Are these methods mutual substitutes or complementary partners? While EALs offer superior precision in locating the apical constriction, radiographs provide indispensable anatomical visualization. This article synthesizes the latest peer-reviewed data to help professionals navigate accuracy, radiation safety, and clinical limitations. The following analysis is for informational purposes and does not constitute individualized clinical advice.
Background – Working Length and Conventional Radiographic Methods
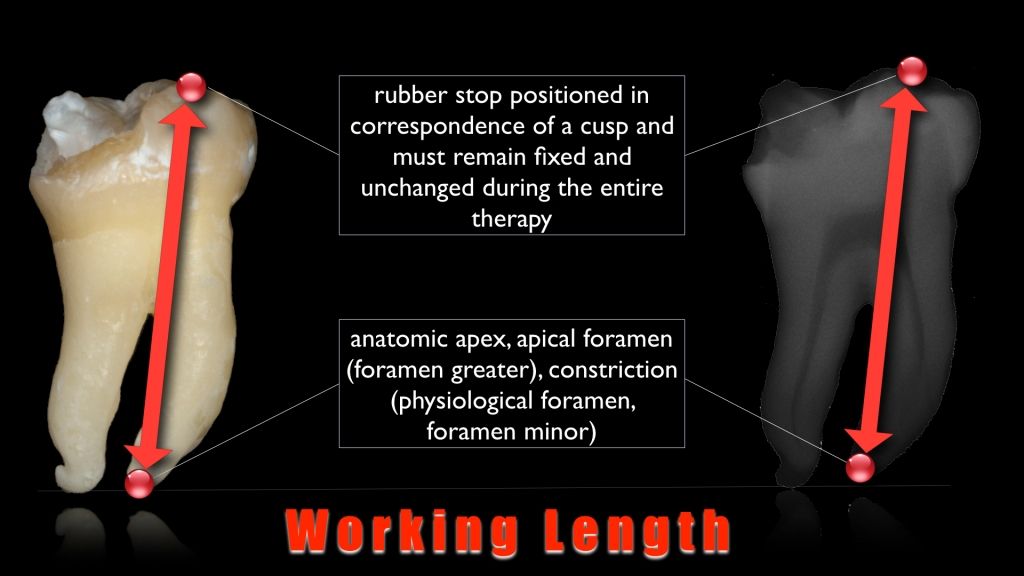
Working length is the distance from a reproducible coronal reference point to a position near the root tip where instrumentation and obturation should end. If this length is significantly underestimated, portions of the canal—especially in the apical third—may remain untreated, increasing the chance of persistent infection. If it is greatly overestimated, files and filling materials may be forced beyond the foramen into peri‑apical tissues, provoking inflammation and compromising healing.
Traditionally, radiographs have been the primary tool for estimating this length. After access, a file is placed to an estimated position, and a working‑length radiograph is taken. The clinician then judges, from a two‑dimensional image, how close the file tip is to the radiographic apex and adjusts the length accordingly. Radiographs offer important anatomical information—such as root curvature, number of roots and the presence of lesions—but they also have inherent limitations: they depict 3D structures in 2D, can be distorted by angulation, and usually require multiple exposures to refine the measurement.
What Is Working Length?
Working length is the distance from a reproducible coronal reference point to a position close to the root apex where canal preparation and obturation are intended to stop. Clinically, this level is usually associated with the apical constriction rather than the radiographic apex. If the working length is underestimated, the apical portion of the canal may remain untreated; if it is greatly overestimated, instruments and filling materials can extend beyond the foramen into peri‑apical tissues and irritate them.
How Radiographs Are Traditionally Used for Working Length
In conventional practice, working length is often established with the help of intra‑oral radiographs. After access and initial canal scouting, a file is placed to an estimated length and a working‑length radiograph is taken. The clinician then evaluates, on a two‑dimensional image, how far the file tip lies from the radiographic apex and adjusts the length accordingly. Additional films may be taken to refine this estimate or to check other canals. Radiographs provide valuable information about root morphology, curvature, number of canals and peri‑apical status, and they are essential for documentation. However, they present 3D anatomy in 2D, are subject to projection errors and often require multiple exposures to approximate the desired working length.
Background – Working Length and Conventional Radiographic Methods
Working length is the distance from a reproducible coronal reference point to a position near the root tip where instrumentation and obturation should end. If this length is significantly underestimated, portions of the canal—especially in the apical third—may remain untreated, increasing the chance of persistent infection. If it is greatly overestimated, files and filling materials may be forced beyond the foramen into peri‑apical tissues, provoking inflammation and compromising healing.
Traditionally, radiographs have been the primary tool for estimating this length. After access, a file is placed to an estimated position, and a working‑length radiograph is taken. The clinician then judges, from a two‑dimensional image, how close the file tip is to the radiographic apex and adjusts the length accordingly. Radiographs offer important anatomical information—such as root curvature, number of roots and the presence of lesions—but they also have inherent limitations: they depict 3D structures in 2D, can be distorted by angulation, and usually require multiple exposures to refine the measurement.
What Is Working Length?
Working length is the distance from a reproducible coronal reference point to a position close to the root apex where canal preparation and obturation are intended to stop. Clinically, this level is usually associated with the apical constriction rather than the radiographic apex. If the working length is underestimated, the apical portion of the canal may remain untreated; if it is greatly overestimated, instruments and filling materials can extend beyond the foramen into peri‑apical tissues and irritate them.
How Radiographs Are Traditionally Used for Working Length
In conventional practice, working length is often established with the help of intra‑oral radiographs. After access and initial canal scouting, a file is placed to an estimated length and a working‑length radiograph is taken. The clinician then evaluates, on a two‑dimensional image, how far the file tip lies from the radiographic apex and adjusts the length accordingly. Additional films may be taken to refine this estimate or to check other canals. Radiographs provide valuable information about root morphology, curvature, number of canals and peri‑apical status, and they are essential for documentation. However, they present 3D anatomy in 2D, are subject to projection errors and often require multiple exposures to approximate the desired working length.
How Electronic Apex Locators Determine Working Length
An electronic apex locator determines working length by analysing the electrical behaviour of a closed circuit formed between the endodontic file inside the canal and a reference electrode, usually a lip hook placed on moist oral mucosa. As the file advances apically, the surrounding tissues and canal contents create characteristic changes in the impedance of this circuit. The device continuously measures that impedance and, through its internal algorithms, interprets when the file tip is approaching and then reaching the region of the apical constriction.
Early models of apex locator relied on simple direct‑current resistance and a fixed “target value” thought to correspond to the apex. Modern devices use alternating current at multiple frequencies and analyse impedance ratios rather than a single resistance reading. This allows them to work more reliably in the presence of irrigants such as NaOCl or EDTA and in canals that are moist rather than completely dry. The unit then converts these electrical measurements into a visual scale and/or audio signals, giving the clinician real‑time feedback on the file tip’s position relative to the apical tissues while shaping the canal.
Overview of Systematic Reviews and Clinical Studies
Over the last two decades, numerous in‑vitro and in‑vivo studies have compared electronic apex locator measurements with radiographic working‑length estimates. Systematic reviews and meta‑analyses generally report that modern EALs are at least as accurate as radiographs, and in many trials more accurate, for locating the apical constriction. A systematic review by Martins et al. (2014), for example, concluded that EAL‑based measurements were closer to the apical constriction than radiographic methods in most included studies. Other reviews and comparative trials published in journals such as the International Endodontic Journal and Journal of Endodontics echo this overall finding, while also noting differences between specific devices and study designs.
Although details vary—model of apex locator, tooth type, irrigants used and whether teeth are in vivo or ex vivo—the consistent pattern is that EALs provide a reliable electronic estimate of working length, particularly when canals are reasonably prepared and moisture is controlled according to the manufacturer’s instructions.
Reported Accuracy Ranges and Clinical Implications
Individual studies often report the proportion of measurements falling within a predefined tolerance, such as ±0.5 mm of the reference length. For many contemporary EALs, reported accuracy within this range commonly lies between about 70% and 95%, whereas radiographic estimates in the same studies tend to show lower percentages or greater variance. Some authors even describe “electronic determination of working length” as more accurate than conventional radiography for locating the minor foramen.
Clinically, these findings suggest that using an electronic apex locator can reduce the likelihood of significant over‑ or under‑estimation of canal length, which in turn may help minimise over‑instrumentation and incomplete cleaning near the apex. However, these percentages are still probabilities, not guarantees; they must be interpreted in light of each case and device.
Quality and Limitations of the Evidence
Despite generally favourable results for the electronic apex locator, several reviews emphasise that the overall certainty of the evidence is low to moderate. Studies differ widely in design, sample size, tooth type, irrigants, reference standards and operator experience. Many are in‑vitro or ex‑vivo investigations that may not fully mirror clinical conditions. As a result, while the data strongly support EALs as accurate tools for working‑length determination, they do not justify abandoning radiographs or clinical judgement in individual cases.
Key Advantages of Electronic Apex Locators over Radiography
More Accurate Location of the Apical Constriction
Radiographs show the radiographic apex, not the narrowest apical constriction, and the two do not always coincide. An electronic apex locator measures bio‑electrical changes as the file tip approaches the apical tissues, so its “zero” point is usually closer to the minor foramen than the image on a film. Many studies on apex locator accuracy report that EAL measurements fall within a narrow tolerance of the apical constriction more often than radiographic estimates. In practice, this means a reduced risk of significant over‑ or under‑estimation of canal length when the device is used correctly and in suitable conditions.
Fewer Radiographs and Reduced Radiation
Because a electronic apex locator can provide a reliable electronic working length, fewer radiographs are usually needed to refine file position. Several clinical papers note that using an apex locator for initial and interim measurements can eliminate multiple “check” films, with radiographs reserved for confirmation and documentation. This does not remove the need for X‑rays altogether, but it does lower cumulative radiation exposure for the patient and can shorten chair time for both dentist and patient.
Convenience in Difficult Clinical Situations
In some situations, placing and angling a film or sensor is technically difficult—for example, in patients with a strong gag reflex, limited mouth opening or very posterior teeth. Metal crowns, posts or orthodontic appliances can also complicate interpretation. In these cases, an electronic apex locator offers a practical way to obtain working‑length information when radiographs alone are awkward or less clear, providing guidance while still allowing films to be taken when feasible.
While the clinical advantages of EALs over radiographs are clear, achieving these results depends on selecting the right equipment and following a standardized clinical protocol. For a comprehensive look at the different generations of devices, a step-by-step usage guide, and an expert buying checklist for 2026, see our primary resource: Electronic Apex Locator: 2026 Guide to Use, Types & Buying.
Limitations of Electronic Apex Locators and the Ongoing Role of Radiographs
Situations Where EAL Readings Are Less Reliable
Although an electronic apex locator performs well in many canals, there are recognised situations where its readings become less reliable. Open or immature apices, extensive apical resorption, large peri‑apical lesions, root perforations and vertical root fractures can all allow current to leak into surrounding tissues earlier than expected, leading to an apex locator false reading that appears shorter or longer than reality. Severely calcified or blocked canals may prevent the file from reaching the region required for accurate measurement, while poor isolation and uncontrolled moisture can also distort values. In these scenarios, authors recommend treating EAL output as limited reference data rather than a stand‑alone answer, and placing greater weight on radiographs and overall clinical findings.
Information Radiographs Still Provide
Even when an electronic apex locator is used for working‑length determination, radiographs remain essential. They provide information that an EAL cannot: the number of roots and canals, degree and direction of curvature, presence of previous fillings or posts, size and location of peri‑apical radiolucencies, and the relationship of instruments and obturation materials to surrounding anatomical structures. Radiographs are also a key part of medico‑legal documentation, showing pre‑operative status, working length confirmation and final root‑filling quality. For these reasons, comparative studies that favour EALs for length measurement still conclude that films are required for diagnosis, treatment planning and outcome assessment. In modern practice, EALs reduce but do not replace radiographs; instead, the two tools are used together to give a more complete picture of each case.
Practical Approach – Combining EALs and Radiographs in Clinical Workflow
In most contemporary protocols, the question is not whether to use an electronic apex locator or radiographs, but how to integrate both. Many clinicians use the apex locator as the primary tool for determining and monitoring working length during canal preparation. The device gives real‑time feedback as the file advances, making it easier to establish an initial length and to check whether that length has changed after further shaping.
Radiographs are then taken at selected stages, rather than every time the file position is adjusted. A common pattern is to obtain a pre‑operative film for diagnosis and planning, use the electronic apex locator to refine working length during treatment, and take one or more working‑length or final films to confirm instrument or filling positions and to document the case. In difficult or atypical anatomy, the relative weight given to EAL readings versus radiographic information is adjusted by the dentist according to training, local guidelines and the specifics of the case. This combined use allows the strengths of each method to complement the other.
Clinical and experimental studies consistently indicate that electronic apex locator devices are at least as accurate as radiographs, and often more so, for locating the apical constriction. Using an apex locator can reduce the number of films needed and lower radiation exposure, while helping to avoid significant over‑ or under‑estimation of canal length. At the same time, radiographs continue to provide essential information about anatomy, pathology and treatment outcome that EALs cannot supply. In everyday practice, the two methods are usually combined, with working‑length estimates from the EAL interpreted and confirmed in the context of radiographic and clinical findings.










